
Six-Minute Walking Test Performance Relates to Neurocognitive Abilities in Preschoolers

 ,
,  ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Outcome Measures
2.2. Procedures
3. Results
3.1. Main Sample
3.2. ERP Subsample
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical activity, fitness, cognitive function, and academic achievement in children: A systematic review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef]
- McLoughlin, G.M.; Bai, Y.; Welk, G.J. Longitudinal Associations between Physical Fitness and Academic Achievement in Youth. Med. Sci. Sports Exerc. 2020, 52, 616–622. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [Green Version]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Chaddock, L.; Erickson, K.I.; Prakash, R.S.; Vanpatter, M.; Voss, M.W.; Pontifex, M.B.; Raine, L.B.; Hillman, C.H.; Kramer, A.F. Basal ganglia volume is associated with Aerobic fitness in preadolescent children. Dev. Neurosci. 2010, 32, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Verburgh, L.; Königs, M.; Scherder, E.J.A.; Oosterlaan, J. Physical exercise and executive functions in preadolescent children, adolescents and young adults: A meta-analysis. Br. J. Sports Med. 2014, 48, 973–979. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Davidson, M.C.; Amso, D.; Anderson, L.C.; Diamond, A. Development of cognitive control and executive functions from 4 to 13 years: Evidence from manipulations of memory, inhibition, and task switching. Neuropsychologia 2006, 44, 2037–2078. [Google Scholar] [CrossRef] [Green Version]
- Raine, L.B.; Kao, S.-C.; Pindus, D.; Westfall, D.R.; Shigeta, T.T.; Logan, N.; Cadenas-Sanchez, C.; Li, J.; Drollette, E.S.; Pontifex, M.B. A large-Scale reanalysis of childhood fitness and inhibitory control. J. Cogn. Enhanc. 2018, 2, 170–192. [Google Scholar] [CrossRef]
- Drollette, E.S.; Scudder, M.R.; Raine, L.B.; Davis Moore, R.; Pontifex, M.B.; Erickson, K.I.; Hillman, C.H. The sexual dimorphic association of cardiorespiratory fitness to working memory in children. Dev. Sci. 2016, 19, 90–108. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Kamijo, K.; Scudder, M.R.; Raine, L.B.; Khan, N.A.; Hemrick, B.; Evans, E.M.; Castelli, D.M.; Frank, K.A.; Hillman, C.H. The differential association of adiposity and fitness with cognitive control in preadolescent children. Monogr. Soc. Res. Child Dev. 2014, 79, 72–92. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Raine, L.B.; Johnson, C.R.; Chaddock, L.; Voss, M.W.; Cohen, N.J.; Kramer, A.F.; Hillman, C.H. Cardiorespiratory fitness and the flexible modulation of cognitive control in preadolescent children. J. Cogn. Neurosci. 2011, 23, 1332–1345. [Google Scholar] [CrossRef]
- Stroth, S.; Kubesch, S.; Dieterle, K.; Ruchsow, M.; Heim, R.; Kiefer, M. Physical fitness, but not acute exercise modulates event-related potential indices for executive control in healthy adolescents. Brain Res. 2009, 1269, 114–124. [Google Scholar] [CrossRef]
- Chaddock-Heyman, L.; Erickson, K.I.; Holtrop, J.L.; Voss, M.W.; Pontifex, M.B.; Raine, L.B.; Hillman, C.H.; Kramer, A.F. Aerobic fitness is associated with greater white matter integrity in children. Front. Hum. Neurosci. 2014, 8, 1–7. [Google Scholar] [CrossRef]
- Tucker, P. The physical activity levels of preschool-aged children: A systematic review. Early Child. Res. Q. 2008, 23, 547–558. [Google Scholar] [CrossRef]
- Becker, D.R.; McClelland, M.M.; Loprinzi, P.; Trost, S.G. Physical activity, self-regulation, and early academic achievement in preschool children. Early Educ. Dev. 2014, 25, 56–70. [Google Scholar] [CrossRef]
- Tomporowski, P.D.; Davis, C.L.; Miller, P.H.; Naglieri, J.A. Exercise and children’s intelligence, cognition, and academic achievement. Educ. Psychol. Rev. 2008, 20, 111–131. [Google Scholar] [CrossRef]
- Wassenberg, R.; Kessels, A.G.H.; Kalff, A.C.; Hurks, P.P.M.; Jolles, J.; Feron, F.J.M.; Hendriksen, J.G.M.; Kroes, M.; Beeren, M.; Vles, J.S.H. Relation between cognitive and motor performance in 5- To 6-year-old children: Results from a large-scale cross-sectional study. Child Dev. 2005, 76, 1092–1103. [Google Scholar] [CrossRef]
- Schmitt, B.M.; Münte, T.F.; Kutas, M. Electrophysiological estimates of the time course of semantic and phonological encoding during listening and naming. Neuropsychologia 2002, 40, 778–787. [Google Scholar] [CrossRef] [Green Version]
- Polich, J. Updating P300: An integrative theory of P3a and P3b. Clin. Neurophysiol. 2007, 118, 2128–2148. [Google Scholar] [CrossRef] [Green Version]
- Hillman, C.; Buck, S.; Themanson, J.; Pontifex, M.; Castelli, D. Aerobic fitness and cognitive development: Event-related brain potential and task performance indices of executive control in preadolescent children. Dev. Psychol. 2009, 45, 114–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillman, C.; Castelli, D.; Buck, S. Aerobic fitness and neurocognitive function in healthy preadolescent children. Med. Sci. Sports Exerc. 2005, 37, 1967–1974. [Google Scholar] [CrossRef] [Green Version]
- Raine, L.B.; Khan, N.A.; Drollette, E.S.; Pontifex, M.B.; Kramer, A.F.; Hillman, C.H. Obesity, visceral adipose tissue, and cognitive function in childhood. J. Pediatr. 2017, 187, 134–140.e3. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, K.; Khan, N.A.; Pontifex, M.B.; Scudder, M.R.; Drollette, E.S.; Raine, L.B.; Evans, E.M.; Castelli, D.M.; Hillman, C.H. The relation of adiposity to cognitive control and scholastic achievement in preadolescent children. Obesity 2012, 20, 2406–2411. [Google Scholar] [CrossRef] [PubMed]
- Morinder, G. Six-minute walk test in obese children and adolescents: Reproducibility and validity. Physiother. Res. Int. Physiother. Res. Int. 2009, 14, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Pathare, N.; Haskvitz, E.M.; Selleck, M. 6-Minute Walk Test Performance in Young Children who are Normal Weight and Overweight. Cardiopulm. Phys. Ther. J. 2012, 23, 12–18. [Google Scholar] [CrossRef]
- Khan, N.A.; Baym, C.L.; Monti, J.M.; Raine, L.B.; Drollette, E.S.; Scudder, M.R.; Moore, R.D.; Kramer, A.F.; Hillman, C.H.; Cohen, N.J. Central adiposity is negatively associated with hippocampal-dependent relational memory among overweight and obese children. J. Pediatr. 2015, 166, 302–308. [Google Scholar] [CrossRef] [Green Version]
- Whitmer, R.A.; Gustafson, D.R.; Barrett-Connor, E.; Haan, M.N.; Gunderson, E.P.; Yaffe, K. Central obesity and increased risk of dementia more than three decades later. Neurology 2008, 71, 1057–1064. [Google Scholar] [CrossRef]
- Georgieff, M.K. Nutrition and the developing brain: Nutrient priorities and measurement. Am. J. Clin. Nutr. 2007, 85, 614S–620S. [Google Scholar]
- Sherry, C.L.; Kim, S.S.; Dilger, R.N.; Bauer, L.L.; Moon, M.L.; Tapping, R.I.; Fahey, G.C., Jr.; Tappenden, K.A.; Freund, G.G. Sickness behavior induced by endotoxin can be mitigated by the dietary soluble fiber, pectin, through up-regulation of IL-4 and Th2 polarization. Brain. Behav. Immun. 2010, 24, 631–640. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.; Dilger, R.N.; Johnson, R.W. Luteolin inhibits microglia and alters hippocampal-dependent spatial working memory in aged mice. J. Nutr. 2010, 140, 1892–1898. [Google Scholar] [CrossRef] [Green Version]
- Hoyland, A.; Lawton, C.L.; Dye, L. Acute effects of macronutrient manipulations on cognitive test performance in healthy young adults: A systematic research review. Neurosci. Biobehav. Rev. 2008, 32, 72–85. [Google Scholar] [CrossRef]
- Khan, N.A.; Raine, L.B.; Drollette, E.S.; Scudder, M.R.; Kramer, A.F.; Hillman, C.H. Dietary Fiber Is Positively Associated with Cognitive Control among Prepubertal. J. Nutr. Ingestive Behav. Neurosci. 2015, 145, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Florence, M.D.; Asbridge, M.; Veugelers, P.J. Diet quality and academic performance. J. Sch. Health 2008, 78, 209–215. [Google Scholar] [CrossRef]
- Geiger, R.; Strasak, A.; Treml, B.; Gasser, K.; Kleinsasser, A.; Fischer, V.; Geiger, H.; Loeckinger, A.; Stein, J.I. Six-minute walk test in children and adolescents. J. Pediatr. 2007, 150, 395–399.e2. [Google Scholar] [CrossRef]
- Lammers, A.E.; Hislop, A.A.; Flynn, Y.; Haworth, S.G. The 6-minute walk test: Normal values for children of 4–11 years of age. Arch. Dis. Child. 2008, 93, 464–468. [Google Scholar] [CrossRef]
- Kervio, G.; Carre, F.; Ville, N. Reliability and intensity of the six-minute walk test in healthy elderly subjects. Med. Sci. Sport. Exerc. 2003, 35, 169–174. [Google Scholar] [CrossRef]
- Burr, J.F.; Bredin, S.S.D.; Faktor, M.D.; Warburton, D.E.R. The 6-minute walk test as a predictor of objectively measured aerobic fitness in healthy working-aged adults. Phys. Sportsmed. 2011, 39, 133–139. [Google Scholar] [CrossRef]
- Li, A.M.; Yin, J.; Yu, C.C.W.; Tsang, T.; So, H.K.; Wong, E.; Chan, D.; Hon, E.K.L.; Sung, R. The six-minute walk test in healthy children: Reliability and validity. Eur. Respir. J. 2005, 25, 1057–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhelst, J.; Fardy, P.S.; Salleron, J.; Béghin, L. The six-minute walk test in obese youth: Reproducibility, validity, and prediction equation to assess aerobic power. Disabil. Rehabil. 2013, 35, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC growth charts: United States. Adv. Data 2000, 314, 1–27. [Google Scholar]
- Micklesfield, L.K.; Goedecke, J.H.; Punyanitya, M.; Wilson, K.E.; Kelly, T.L. Dual-energy X-ray performs as well as clinical computed tomography for the measurement of visceral fat. Obesity 2012, 20, 1109–1114. [Google Scholar] [CrossRef]
- Khan, N.A.; Cannavale, C.; Iwinski, S.; Liu, R.; McLoughlin, G.M.; Steinberg, L.G.; Walk, A.M. Visceral adiposity and diet quality are differentially associated with cognitive abilities and early academic skills among preschool-age children. Front. Pediatr. 2020, 7, 548. [Google Scholar] [CrossRef] [Green Version]
- ATS Board of Directors. American thoracic society ATS statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Laforte, E.M.; Mcgrew, K.S.; Schrank, F.A. Woodcock-Johnson ® IV Tests of Early Cognitive and Academic Development: Overview and Technical Abstract (Woodcock-Johnson IV Assessment Service Bulletin No 4); Riverside: Rolling Meadows, IL, USA, 2015; ISBN 800.323.9540. [Google Scholar]
- Eriksen, B.A.; Eriksen, C.W. Effects of noise letters upon identification of a target letter in a non-search task. Percept. Psychophys. 1974, 16, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Zelazo, P.D.; Anderson, J.E.; Richler, J.; Wallner-Allen, K.; Beaumont, J.L.; Weintraub, S. NIH toolbox cognition battery (CB): Measuring executive function and attention. Monogr. Soc. Res. Child Dev. 2013, 78, 16–33. [Google Scholar] [CrossRef]
- Khan, N.A.; Hillman, C.H. The relation of childhood physical activity and aerobic fitness to brain function and cognition: A review. Pediatr. Exerc. Sci. 2014, 26, 138–146. [Google Scholar] [CrossRef]
- Luck, S.J.; Gaspelin, N. How to get statistically significant effects in any ERP experiment (and why you shouldn’t). Psychophysiology 2017, 54, 146–157. [Google Scholar] [CrossRef] [Green Version]
- Tomé, D.; Barbosa, F.; Nowak, K.; Marques-Teixeira, J. The development of the N1 and N2 components in auditory oddball paradigms: A systematic review with narrative analysis and suggested normative values. J. Neural Transm. 2015, 122, 375–391. [Google Scholar] [CrossRef] [Green Version]
- Niederer, I.; Kriemler, S.; Gut, J.; Hartmann, T.; Schindler, C.; Barral, J.; Puder, J.J. Relationship of aerobic fitness and motor skills with memory and attention in preschoolers (Ballabeina): A cross-sectional and longitudinal study. BMC Pediatr. 2011, 11. [Google Scholar] [CrossRef] [Green Version]
- Chaddock-Heyman, L.; Erickson, K.I.; Kienzler, C.; King, M.; Pontifex, M.B.; Raine, L.B.; Hillman, C.H.; Kramer, A.F. The role of aerobic fitness in cortical thickness and mathematics achievement in preadolescent children. PLoS ONE 2015, 10, 1–11. [Google Scholar] [CrossRef]
- Álvarez-Bueno, C.; Hillman, C.H.; Cavero-Redondo, I.; Sánchez-López, M.; Pozuelo-Carrascosa, D.P.; Martínez-Vizcaíno, V. Aerobic fitness and academic achievement: A systematic review and meta-analysis. J. Sports Sci. 2020, 38, 582–589. [Google Scholar] [CrossRef]
- Hillman, C.; Kamijo, K.; Pontifex, M. The relation of ERP indices of exercise to brain health and cognition. In Functional Neuroimaging in Exercise; Springer: New York, NY, USA, 2012; pp. 419–446. ISBN 9781461432937. [Google Scholar]
- Polich, J.; Lardon, M. P300 and long-term physical exercise. Electroencephalogr. Clin. Neurophysiol. 1997, 103, 493–498. [Google Scholar] [CrossRef]
- Chang, Y.-K.; Tsai, Y.-J.; Chen, T.-T.; Hung, T.-M. The impacts of coordinative exercise on executive function in kindergarten children: An ERP study. Exp. Brain Res. 2013, 225, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Burdette, H.L.; Whitaker, R.C. Resurrecting free play in young children. Arch. Pediatr. Adolesc. Med. 2005, 159, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krafft, C.E.; Schaeffer, D.J.; Schwarz, N.F.; Chi, L.; Weinberger, A.L.; Pierce, J.E.; Rodrigue, A.L.; Allison, J.D.; Yanasak, N.E.; Liu, T.; et al. Improved frontoparietal white matter integrity in overweight children is associated with attendance at an after-school exercise program. Dev. Neurosci. 2014, 36, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | Minimum | Maximum | |
|---|---|---|---|
| Sex, Females/Males | 25/34 (42% female) | ||
| Age, years | 5.0 ± 0.6 | 4.0 | 6.0 |
| Race (n = 51) | |||
| Asian, n (%) | 6 (9.5) | ||
| Black/African American, n (%) | 3 (4.8) | ||
| White or Caucasian, n (%) | 34 (54) | ||
| Mixed or Other, n (%) | 8 (12.7) | ||
| Household Income (n = 52) | |||
| <10,000–40,000, n (%) | 12 (19) | ||
| 41,000–80,000, n (%) | 12 (19) | ||
| ≥81,000, n(%) | 28 (44.4) | ||
| BMI-for-age %ile | 51.8 ± 33.7 | 0.1 | 99.9 |
| Underweight, n (%) | 4 (7) | ||
| Normal or Healthy, n (%) | 40 (70) | ||
| Overweight, n (%) | 4 (7) | ||
| Obese, n (%) | 9 (16) | ||
| Visceral Adipose Tissue (n = 53) | 113.6 ± 65.8 | 4.1 | 234.5 |
| Total Healthy Eating Index-2015 (n = 55) | 54.2 ± 14.2 | 24.3 | 92.0 |
| Woodcock Johnson ECAD™ (n = 53) | |||
| General Intellectual Ability | 109.1 ± 14.2 | 76 | 141 |
| Early Academic Skills | 101.4 ± 14.3 | 72 | 138 |
| Expressive Language | 110.3 ± 16.0 | 76 | 143 |
| Flanker Task (n = 48) | |||
| Congruent Accuracy, % | 65.4 ± 24.2 | 5 | 97.5 |
| Congruent Reaction Time, ms | 1246.8 ± 208.6 | 661.3 | 1629.5 |
| Incongruent Accuracy, % | 54.2 ± 24.2 | 7.5 | 100 |
| Incongruent Reaction Time, ms | 1293.8 ± 276.5 | 455.6 | 1781.8 |
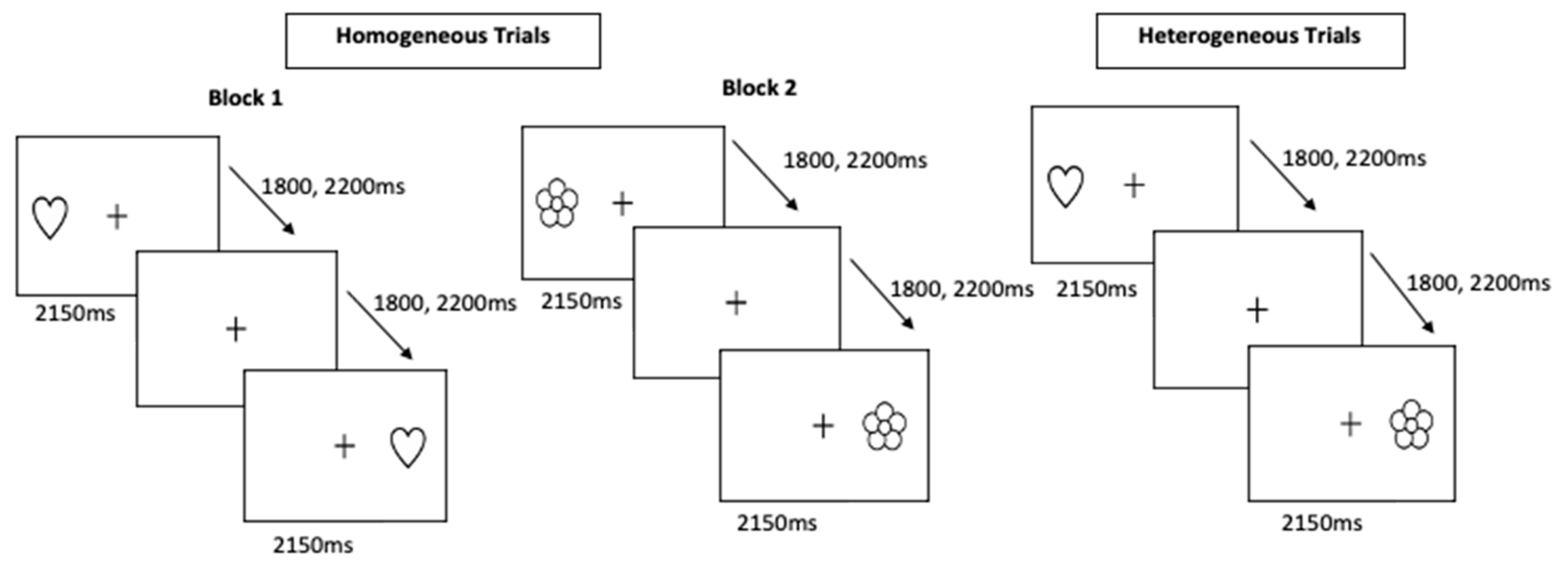
| Hearts and Flowers Task (n = 53) | |||
| Homogeneous Accuracy, % | 76.7 ± 17.3 | 20 | 100 |
| Homogeneous Reaction Time, ms | 945.0 ± 198.5 | 444.5 | 1318.5 |
| Heterogeneous Accuracy, % | 59.4 ± 21.6 | 10 | 95 |
| Heterogeneous Reaction Time, ms | 1137.5 ± 216.4 | 484.5 | 1537.4 |
| 6-Minute Walking Test (n = 59) | |||
| Total Distance Walked, m | 449.6 ± 82.0 | 240 | 600 |
| Heart Rate (pre-test), bpm | 97.3 ± 19.2 | 53 | 152 |
| Heart Rate (post-test), bpm | 132.3 ± 24.2 | 67 | 178 |
| Oxygen Saturation (pre-test), % | 97.6 ± 2.2 | 89 | 100 |
| Oxygen Saturation (post-test), % | 97.2 ± 2.0 | 92 | 100 |
| β | Coefficient P | R2 | Adjusted R2 | Model P | ||
|---|---|---|---|---|---|---|
| Woodcock Johnson Early Cognitive and Academic Development Test (n = 53) | General Intellectual Ability | 0.06 | 0.04 | 0.04 | ||
| 6MWT Distance Walked | 0.25 * | 0.04 | ||||
| Early Academic Skills | 0.13 | 0.09 | 0.05 | |||
| Visceral Adipose Tissue | −0.22 | 0.14 | ||||
| 6MWT Distance Walked | 0.25 | 0.09 | ||||
| Expressive Language | 0.16 | 0.13 | 0.02 | |||
| Healthy Eating Index-2015 | 0.27 * | 0.05 | ||||
| 6MWT Distance Walked | 0.30 * | 0.04 | ||||
| Flanker Task (n = 48) | Congruent Accuracy | 0.24 | 0.18 | <0.01 | ||
| Sex | 0.29 | 0.02 | ||||
| General Intellectual Ability | 0.25 | 0.04 | ||||
| 6MWT Distance Walked | 0.29 * | 0.02 | ||||
| Congruent Reaction Time | 0.14 | 0.08 | 0.04 | |||
| Age | −0.18 | 0.12 | ||||
| Sex | −0.26 * | 0.04 | ||||
| 6MWT Distance Walked | −0.16 | 0.14 | ||||
| Incongruent Reaction Time | 0.07 | 0.05 | 0.04 | |||
| 6MWT Distance Walked | −0.26 * | 0.04 | ||||
| Hearts and Flowers Task (n = 53) | Homogeneous Accuracy | 0.24 | 0.21 | <0.01 | ||
| Age | 0.37 * | <0.01 | ||||
| 6MWT Distance Walked | 0.23 * | 0.04 | ||||
| Homogeneous Reaction Time | 0.17 | 0.14 | 0.01 | |||
| Age | −0.32 * | 0.01 | ||||
| 6MWT Distance Walked | −0.19 | 0.09 | ||||
| Heterogeneous Accuracy | 0.43 | 0.40 | <0.01 | |||
| Age | 0.43 * | <0.01 | ||||
| General Intellectual Ability | 0.29 * | 0.01 | ||||
| 6MWT Distance Walked | 0.26 * | 0.02 | ||||
| Heterogeneous Reaction Time | <0.01 | <0.01 | 0.39 | |||
| 6MWT Distance Walked | −0.04 | 0.39 |
| M | SD | Minimum | Maximum | |
|---|---|---|---|---|
| Participant Characteristics (n = 26) | ||||
| Age, years | 5.08 | 0.54 | 4.2 | 6.0 |
| Sex, Females/Males | 16, 10 | |||
| 6-Minute Walking Test | ||||
| Total Distance Walked, m | 465.50 | 68.39 | 289.7 | 580 |
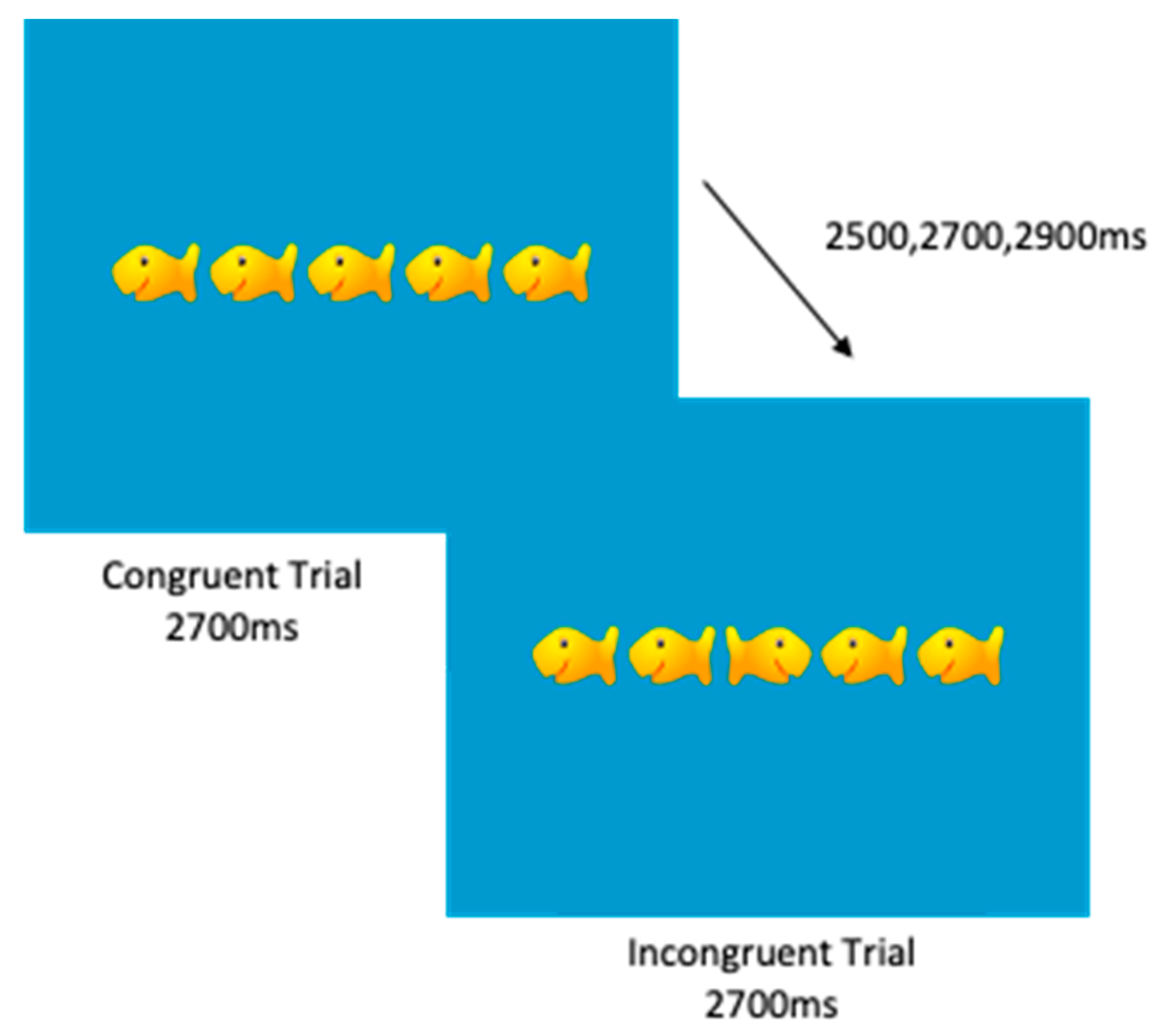
| Oddball Task Performance | ||||
| Accuracy for Targets (%) | 75.26 | 18.23 | 27.5 | 97.5 |
| Reaction Time to Targets (ms) | 838.62 | 167.68 | 523.3 | 1115.3 |
| Inverse Efficiency for Targets | 12.20 | 5.12 | 6.1 | 28.0 |
| Coefficient of Variation for Targets | 0.38 | 0.11 | 0.21 | 0.64 |
| ERP Indices | ||||
| Total Target Trials Used (of 40) | 25.19 | 10.65 | 9.0 | 40.0 |
| Artifact Free Trials | 106.7 | 38.6 | 49.0 | 157.0 |
| N2 Mean Amplitude Modulation | 2.51 | 13.77 | −25.0 | 34.4 |
| N2 Peak Latency Modulation | −17.08 | 149.41 | −312.0 | 266 |
| P3 Mean Amplitude Modulation | 4.17 | 14.80 | −23.4 | 36.2 |
| P3 Peak Latency Modulation | −38.08 | 142.73 | −348.0 | 266.0 |
| Correlation with 6MWT Distance Walked | |||
|---|---|---|---|
| Cognitive Task Performance | Pearson r | p-Value | |
| Accuracy for Targets (%) | 0.075 | 0.754 | |
| Reaction Time to Targets (ms) | 0.388 | 0.061 † | |
| Target Inverse Efficiency | 0.058 | 0.787 | |
| Target Coefficient of Variation | −0.361 | 0.083 † | |
| ERP Indices | N2 Mean Amplitude | ||
| Modulation | 0.325 | 0.122 | |
| Target | 0.233 | 0.274 | |
| Standard | −0.113 | 0.559 | |
| N2 Peak Latency | |||
| Modulation | −0.231 | 0.277 | |
| Target | −0.392 | 0.058 † | |
| Standard | −0.109 | 0.614 | |
| P3 Mean Amplitude | |||
| Modulation | 0.361 | 0.083 † | |
| Target | 0.370 | 0.075 † | |
| Standard | −0.004 | 0.985 | |
| P3 Peak Latency | |||
| Modulation | −0.093 | 0.665 | |
| Target | 0.212 | 0.320 | |
| Standard | 0.341 | 0.103 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keye, S.A.; Walk, A.M.; Cannavale, C.N.; Iwinski, S.; McLoughlin, G.M.; Steinberg, L.G.; Khan, N.A. Six-Minute Walking Test Performance Relates to Neurocognitive Abilities in Preschoolers. J. Clin. Med. 2021, 10, 584. https://doi.org/10.3390/jcm10040584
Keye SA, Walk AM, Cannavale CN, Iwinski S, McLoughlin GM, Steinberg LG, Khan NA. Six-Minute Walking Test Performance Relates to Neurocognitive Abilities in Preschoolers. Journal of Clinical Medicine. 2021; 10(4):584. https://doi.org/10.3390/jcm10040584
Chicago/Turabian StyleKeye, Shelby A., Anne M. Walk, Corinne N. Cannavale, Samantha Iwinski, Gabriella M. McLoughlin, Linda G. Steinberg, and Naiman A. Khan. 2021. "Six-Minute Walking Test Performance Relates to Neurocognitive Abilities in Preschoolers" Journal of Clinical Medicine 10, no. 4: 584. https://doi.org/10.3390/jcm10040584